
Getting healthier by reducing risks of coronary artery disease
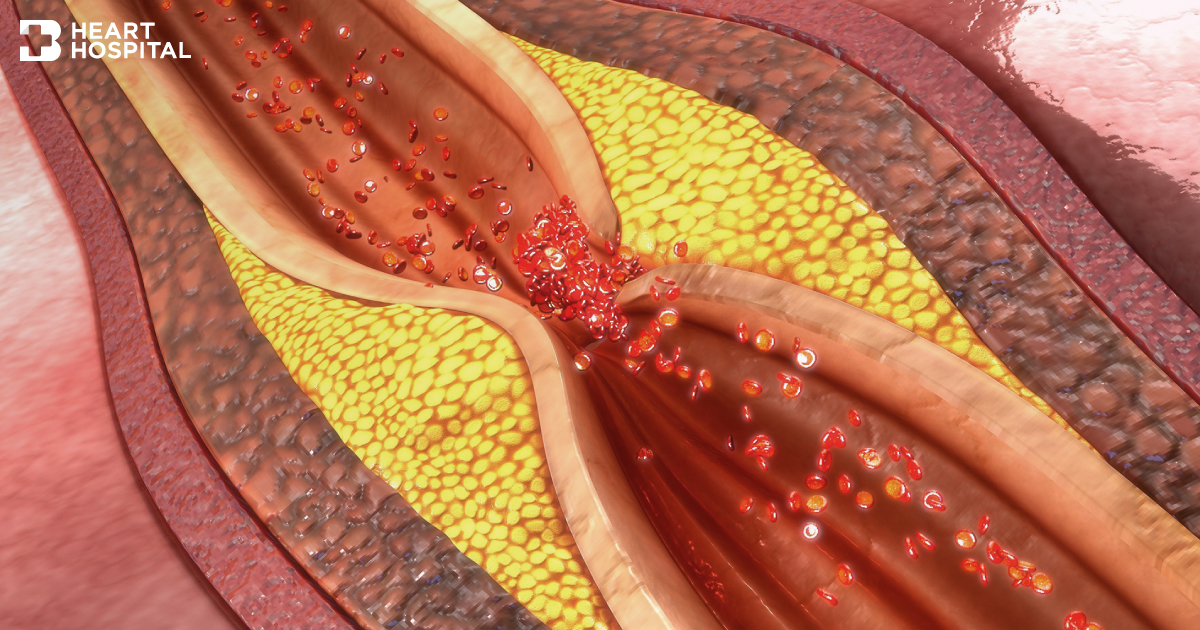
“Coronary artery disease or CAD” is defined as the narrowing or blockage of the coronary arteries, usually caused by atherosclerotic plaque which is made of fat, cholesterol, calcium and other cellular substances that tend to accumulate on the inner walls of the arteries. When plaque builds up, it narrows coronary arteries, resulting in decreased blood flow to the heart. Insufficient blood flow may cause chest pain (angina), shortness of breath or other coronary artery disease signs and symptoms. The lack of blood flow to the heart may damage heart muscles, leading to the condition called “myocardial infarction” with greater risks of developing fatal conditions such as sudden death or heart failure.
The damaged arteries may be caused by various factors including high cholesterol, high blood pressure, diabetes and related lifestyles factors such as being obese or overweight, smoking, physical inactivity, high stress and unhealthy diets e.g. food with trans fat, salt and sugar. Due to this the major contribution of unhealthy lifestyle habits, coronary artery disease has exhibited increased incidences across the world including in Thai population, despite a decline in mortality rates. Thus, lifestyle modifications and being aware of signs and symptoms remain crucial to substantially reduce risks and severity of coronary heart disease.
Causes of coronary artery disease
The heart receives its own supply of blood from the coronary arteries. There are two major coronary arteries branch off from the aorta; left main coronary artery and right coronary artery. These arteries and their branches supply blood to all parts of the heart and heart muscle. The size of small vessels range from 2-4 mm. Once the inner wall of the vessel is injured, atherosclerotic plaque made of fat, cholesterol, calcium and other cellular substances tend to accumulate at the site of injury. When plaque builds up, it narrows the vessel and results in decreased blood supply to the heart and the heart muscle. As a consequence, this leads to insufficient blood supply to heart muscle, causing damaged or dead muscle, called myocardial infarction (heart attack).

Signs and symptoms of coronary artery disease
In the early phase, the decreased blood flow may not cause any coronary artery disease symptoms. As plaque continues to build up in the coronary arteries, patients usually exhibit coronary artery disease signs and symptoms, including:
- Chest pain (angina) or tightness in the chest with unidentified position. However, this pain usually occurs on the middle or left side of the chest or might radiate to the left jaw or arm. It is generally triggered by physical or emotional stress.
- Shortness of breath or extreme fatigue with exertion.
- Epigastric pain radiating to the neck or jaw
Risk factors
With the correlation of atherosclerotic plaque formation, high levels of cholesterol in the blood can significantly increase the risk of formation of plaque and atherosclerosis. High cholesterol can be caused by a high level of low-density lipoprotein (LDL) cholesterol, known as the bad cholesterol. A low level of high-density lipoprotein (HDL) cholesterol, known as the good cholesterol, can also contribute to the development of atherosclerosis. The damaged arteries may be caused by other contributing factors including high blood pressure, diabetes and related lifestyles factors such as being obese or overweight, smoking, physical inactivity, high stress and unhealthy diets.
Uncontrolled high blood pressure can substantially result in hardening and thickening of the arteries, narrowing the channel through which blood can flow. In patients diagnosed with coronary artery disease, pulse rate must be kept between 60 to 70 beats per minute while systolic blood pressure should remain at the range of 120-140 mmHg, not exceed 150 mmHg to minimize the pressure impact on the inner wall of the arteries.
Diagnosis of coronary artery disease
Apart from taking medical history and full physical exam, tests and procedures to diagnose coronary artery disease include:
- Electrocardiogram (ECG). An electrocardiogram is a test that checks how heart functions by measuring the electrical activity of the heart. An ECG can often reveal evidence of heart attack.
- Echocardiogram. An echocardiogram (echo) is a test used to assess the heart’s function and structures. It uses sound waves to produce images of the heart. During an echocardiogram, all parts of the heart wall and pumping activity can be thoroughly examined.
- Exercise Stress Echocardiogram. If signs and symptoms frequently present during exercise, stress tests may be required by walking on a treadmill or riding a stationary bike during an echocardiogram. In some cases, dopamine, medication to stimulate the heart may be used instead of exercise.
- Imaging tests such as cardiac CT scan to evaluate calcium deposits in the arteries and risks of coronary artery disease.
Nevertheless, an ideal test to visualize the arteries is called cardiac catheterization and angiogram. To view blood flow through the heart, a special dye is injected into the coronary arteries (known as an angiogram). During cardiac catheterization, the dye is injected into the arteries of the heart through a long, thin, flexible tube (catheter) that is threaded through an artery, usually in the leg or arm, to the arteries in the heart. The dye outlines narrow spots and blockages on the X-ray images.
Treatment of coronary artery disease
Treatment for coronary artery disease depends on presenting symptoms, degree of blockage and the disease severity. Treatment usually involves lifestyle changes and, if necessary, medications and certain medical procedures including angioplasty, stent placement and surgery.
In case of minor coronary artery disease defined as less than 50-60% artery obstruction, the first-line therapy involves lifestyle changes and medications such as cholesterol-modifying medications, drugs that slow heart rate and decrease blood pressure and aspirin.
In moderate or severe coronary artery disease with greater than 60-70% artery obstruction, balloon angioplasty and stent placement are highly recommended. These procedures significantly help to restore and improve blood flow to the damaged arteries. Balloon angioplasty is a minimally invasive procedure to widen narrowed or obstructed arteries. During the procedure, a long, thin tube (guiding catheter) that has a small balloon on its tip is inserted into the narrowed part of the artery through vessels in the groins or arms. A wire with a deflated balloon is passed through this catheter to the narrowed or blocked area. The balloon is then inflated, compressing the deposits against the artery walls and opening the blocked arteries, resulting in restored blood flood to the heart. After inflation, balloon is then removed. In case of severe blockage, angioplasty is often combined with the permanent placement of a stent, a small wire mesh tube to help opening the arteries and decreasing the chance of narrowing again.
In addition, heart surgery might be considered if several affected arteries are found or the narrowed arteries locate in the area where angioplasty and stent placement are not allowed to effectively and safely perform. The appropriate treatment will be determined by severity of blockage, locations, patient’s individual conditions and relative risks. In case of complicated disease e.g. multiple narrowed coronary arteries, coronary artery bypass surgery might be a superior option.
Coronary artery bypass grafting (CABG)
A cardiothoracic surgeon creates a graft to bypass blocked coronary arteries using a vessel from another part of the body, usually vein from the leg. This allows blood to sufficiently flow around the blocked or narrowed artery. There are 2 main types of CABG; on-pump CABG and off-pump CABG.
- On-pump CABG: During surgery, patient’s heart is stopped temporarily and cardiopulmonary bypass machine (heart-lung machine) is used to keep the blood circulating through the body.
- Off-pump CABG: Off-pump coronary artery bypass or “beating heart” surgery is a form of coronary artery bypass graft (CABG) surgery performed without cardiopulmonary bypass machine. By using local stabilization devices, it allow the rest of the heart to work without disruptions.
Recently, a number of clinical researches especially in the US have revealed that off-pump CABG delivers significant benefits to patients with impaired heart muscle functions, kidney impairments and the elderly with previous history of cerebrovascular disease such as strokes.
In addition, during on-pump CABG with the use of cardiopulmonary bypass machine, required dose of antiplatelet drug becomes tripled. This might potentially lead to blood loss and severe bleeding. With our years of expertise, our cardiothoracic surgeons at Bangkok Heart Hospital have performed off-pump CABG procedure more than thousand cases with close-to-zero 1.2% mortality rate. The oldest patient is 92 years old while patient with the lowest ejection fraction (EF), the percentage of blood that is pumped or ejected out of the ventricles with each contraction remained only 8%.
Prevention of coronary artery disease
Not only to prevent the disease developing in the fist place, lifestyle modifications can significantly help to prevent disease recurrence after receiving treatments. Apart from following the instructions given by the doctors, to improve heart health, recommendations are:
- Eat a low-fat and low-salt diet that is rich in fruits, vegetables, fish and whole grains
- Stay physically active and have regular exercise
- Reduce and manage excessive stress
- Quit smoking and alcohol
- Control medical conditions such as high blood pressure, high cholesterol and diabetes
- Maintain a healthy weight

