Coronary Artery Calcium Scan (CAC) – A test to detect calcified plaque on the walls of the heart’s arteries

Atherosclerosis of Coronary Artery
Coronary Artery Calcium Scan (CAC) is an imaging test used to detect the atherosclerotic plaque that forms on the artery walls of the heart. This plaque is made up of calcium, fats, cholesterol and other substances. Over time, plaque buildup hardens and narrows the arteries, resulting in limited blood flow to the heart and other parts of the body. This plaque can burst, triggering a blood clot and causing life-threatening events such as heart attack.
Atherosclerosis results from chronic inflammation and damages of the inner lining of artery walls. It is a slow, progressive disease that usually takes at least 2-5 years. Damages or injuries to the inner layer of an artery is often caused by diabetes, high blood pressure, high blood lipids e.g. cholesterol and triglycerides, smoking, obesity or overweight and genetic influence. Once the inner wall of the arteries is damaged, blood cells and other substances clump at the injury site, causing the plaque buildup in the inner lining of the arteries. As a result, plaque as a sticky mixture of fatty streaks and calcium reduces the elasticity of the arteries and narrows the artery walls, leading to restricted blood flow.
The presence of plaque on the artery walls is strongly associated with atherosclerosis. Coronary Artery Calcium Scan by using computerized tomography (CT) has been used to detect an atherosclerotic plaque, especially in chronic cases. Nevertheless, this imaging test might not be applicable to identify plaque in acute cases in which lesions might be afresh developed.
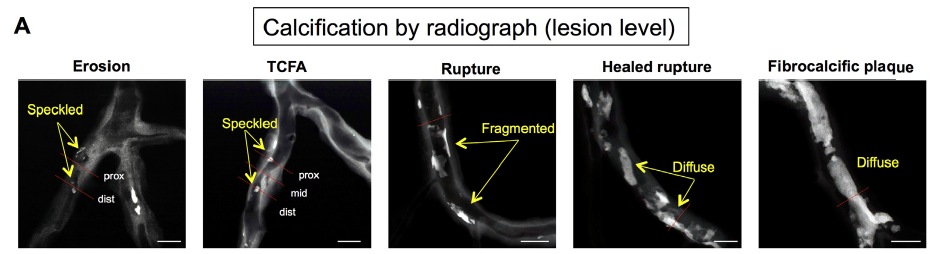
Characterization of calcification based on lesion levels
Calcium deposits on the artery wall are formed as follows:
- Calcium starts accumulating as individual fine speckles or small fragmented lesions (sized 0.5 – 15.0 µm). This is defined as acute lesion that puts patients at risk of acute myocardial infarction (heart attack) and coronary artery disease with high degree of occlusion.
- When calcium accumulates with higher amount, it is shown as clustered line, called diffuse calcification.
- After calcium accumulations fuse and become a calcified patch, it turns to be sheet of calcification sized larger than 3 mm. This stage refers to chronic atherosclerosis.
In summary, plaque characterization e.g. fine speckles, diffuse or sheet patterns can be used to determine whether the detected plaque is freshly developed or chronic one.
Testing and diagnosis
Since thickened or narrowed arteries cause reduced blood flow to the heart, patients often experience chest pain due to insufficient blood supply. Coronary Artery Calcium Scan is considered an effective imaging test to detect atherosclerotic plaque on the artery walls. Since this test is non-invasive, contrast media administration is not required. The test takes approximately 10-15 minutes. Coronary Artery Calcium Scan is able to detect atherosclerotic plaque, therefore the risk of developing myocardial infarction (heart attack) caused by atherosclerosis can be assessed. Combined with other contributing factors as well as clinical signs and symptoms, treatments can be planned accordingly in a timely manner.
Who should have Coronary Artery Calcium Scan
This test is highly recommended in people who are classified into mild to moderate risk groups, including people who have/are:
- Family history of cardiovascular disease
- Men aged over 40
- Women aged over 50 or postmenopausal women
- High blood pressure
- Diabetes
- Obese or overweight
- High blood lipids e.g. cholesterol and triglyceride
- Smokers
*** In high risk group people, people who have had chest pain or shortness of breath or extreme fatigue and patients diagnosed with coronary artery disease, Coronary Artery Calcium Scan might not provide significant benefits. Additional tests or interventions in this group should be furthered conducted by expert cardiologists.

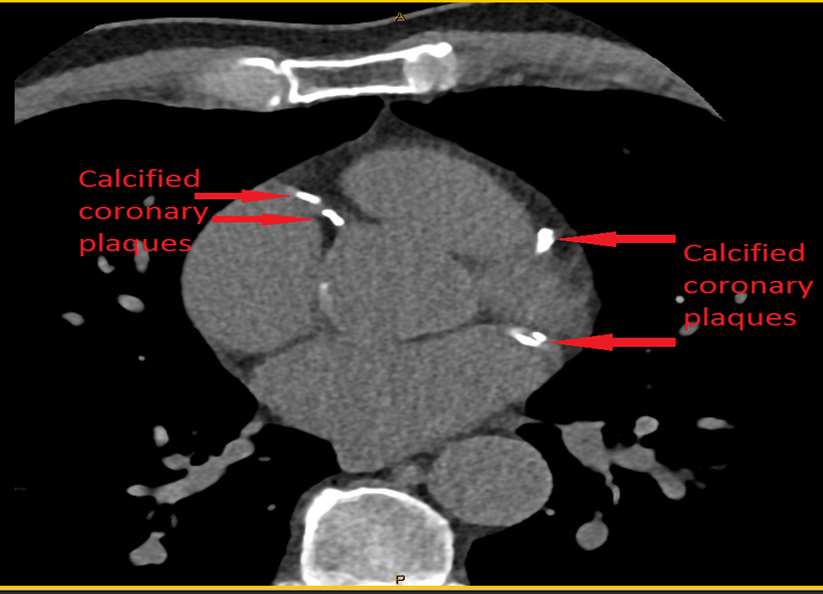
How to conduct Coronary Artery Calcium Scan
To determine calcium scoring, Coronary Artery Calcium Scan employs multidetector or multislice computerized tomography (CT) which is the use of special x-ray equipment to produce multiple detailed pictures of the coronary arteries in order to determine if they are blocked or narrowed by the buildup of plaque. Calcium scoring measures the accumulation levels of plaque which consists of fats, cholesterol, calcium and other substances in the blood. The plaque gradually develops. If it significantly progresses, the sheet or patch of calcification can be clearly detected.
Risks related to Coronary Artery Calcium Scan
Since this test takes only 10-15 minutes and uses very low dose of radiation (approximately 1 millisievert), therefore risks or undesirable effects are considerably low.
Instructions prior to the test
- Food and fluid restrictions are not required.
- Substances such as caffeinated beverages e.g. coffee and tea or medications that raise heart rate or pulse rate should be avoided.
- Smoking must be avoided at least 4 hours before starting the test.
- Patient gown is required to be worn during the test.
- All accessories and jewelry in the neck and chest must be removed.
During the test
- Electrocardiogram (EKG or ECK) is used to monitor and record heart rate and rhythms.
- Patients are instructed to lie down on their backs and hold their breath for 2-10 seconds. During the test, patients should stay still in order to obtain highly clear images.
- In case that patients develop a rapid or fast heartbeat, the cardiologist might consider administrating certain drugs to control their heart rate until it falls within normal range.
- The entire process takes 10-15 minutes.
Instructions after the test
No special instruction is needed after the test. Patients are allowed to continue their normal lives and activities.
Interpretation of the test
The measurement of calcified plaque derived from the test is firmly correlated to the risk of developing coronary artery disease in the future. As the amount of calcium detected increases, the risk of heart attack relatively increases. The interpretation of calcium scoring is principally made by using Agatston Score, a semi-automated tool to calculate a score based on the extent of coronary artery calcification detected by CT scan. Grading of coronary artery disease (based on total calcium score) includes:
- Calcium score 0: No identifiable calcified plaque on the artery wall in the heart. The chance of heart attack or myocardial infarction and coronary artery disease with high degree of occlusion in the future is very low. Recommendation mainly involves the maintenance of healthy diet and lifestyle.
- Calcium score 1-100: A minimal to mild plaque burden is detected in the artery wall and the chance to develop coronary artery conditions is unlikely or considerably low. Maintenance healthy diet and lifestyle is fundamentally advised.
- Calcium score 101 – 400: A moderate plaque burden is detected on the lining of the artery wall and it possesses moderate to high risk of developing heart attack or myocardial infarction and coronary artery disease with high degree of occlusion. Besides significant lifestyle changes, certain medications are additionally suggested under close supervision of expert cardiologists.
- Calcium score greater than 400: An extensive plaque burden is found and atherosclerosis might be strongly indicated with extremely high risk of developing heart attack or myocardial infarction and coronary artery disease with high degree of occlusion. With or without symptoms, additional tests, interventions and treatments are further required under close supervision of expert cardiologists.
| CAC Score | 10 – Year Mortality Risk | Guidance Reassure |
| 0 | Very Low (<1%) | Reassure; maintenance of healthy diet and lifestyle. |
| 1 – 100 | Low (<10%) |
Maintenance of healthy diet and
lifestyle
|
| 101 – 400 | Moderate (10–20%) | Aspirin recommended Statins considered reasonable |
| 101-400 & >75th centile | Moderately High (15-20%) | Reclassify as high risk Aspirin recommended Statins considered reasonable |
| >400 | High (>20%) | Aspirin recommended Statin recommended, to achieve target LDL <2.0 mmol/L Consider functional assessment. |
| * Suggested management based on CAC results for asymptomatic patients | ||
Source: 2017 CSANZ Calcium Score Position Statement