
Atrial fibrillation

What is atrial fibrillation?
Atrial fibrillation is a heart condition with irregular and often abnormally fast heart rate.
A normal heart rate should be between 60 and 100 beats a minute when you’re resting, and is regular. You can measure your heart rate by feeling the pulse in your wrist or neck. In atrial fibrillation, the heart rhythm is irregular and the heart rate may be over 140 beats a minute, although it can be any rate.
Normal, (regular rhythm)

Atrial fibrillation (AF)
(Rapid irregular rhythm)
Atrial fibrillation, or AF, is the most common type of arrhythmia.
Classification of atrial fibrillation
- Paroxysmal atrial fibrillation – this comes and goes and usually stops within 48 hours without any treatment.
- Persistent atrial fibrillation – this lasts for longer than seven days (or less when it is treated).
- Longstanding persistent atrial fibrillation – this means you have had continuous atrial fibrillation for a year or longer.
- Permanent atrial fibrillation – atrial fibrillation is present all the time and no more attempts to restore normal heart rhythm will be made.
Symptoms of atrial fibrillation
Some people with atrial fibrillation have no symptoms and are unaware of their condition until it’s discovered during a physical examination for other purpose. Those who do have atrial fibrillation symptoms may experience signs and symptoms such as:
- Palpitations, which are sensations of a racing, uncomfortable, irregular heartbeat or a flip-flopping in your chest
- Weakness
- Reduced ability to exercise
- Fatigue
- Lightheadedness, dizziness
- Confusion
- Shortness of breath
- Chest pain
Causes of atrial fibrillation
The cause is not fully understood, but it tends to occur in certain groups of people (see below) and may be triggered by certain situations, such as drinking excessive amounts of alcohol, caffeine products.
Atrial fibrillation can affect adults of any age. It affects more men than women and becomes more common in aging population. It affects about 10% of people over 75.
Atrial fibrillation is associated or caused by
- Heart conditions
- Hypertension (high blood pressure)
- Coronary artery disease
- Heart valve disease
- After heart surgery
- Heart failure
- Cardiomyopathy
- Congenital heart disease
- Non heart conditions
- Aging population.
- Obesity, sleep apnea.
- Diabetes
- Pulmonary embolism
- Chronic lung disease
- Hyperthyroidism
- Pericarditis
- Viral infection
In at least 10 percent of the cases, no underlying heart disease is found, a condition called lone atrial fibrillation. In lone atrial fibrillation, the cause is often unclear, and serious complications are rare. In these cases, AF may be related to alcohol or excessive caffeine use, stress, certain drugs, electrolyte or metabolic imbalances, severe infections, or genetic factors.
Atrial fibrillation Complications
AF has two major complications—stroke and heart failure.
- Stroke
During AF, There is stasis of blood in the heart’s upper chambers, the atria. A blood clot (also called a thrombus) can form. If the clot breaks off and travels to the brain, it can cause a stroke. - Heart Failure
Sustain rapid heart beat can cause weakening of the heart muscle. There is also fluid buildup in the body and in the lung causing heart failure symptoms such as shortness of breath, fatigue, legs swelling and weight gain.
How Is Atrial fibrillation Diagnosed?
Atrial fibrillation (AF) is diagnosed based on your medical and family histories, a physical exam, and the results from tests.
Diagnostic Tests and Procedures
- EKG (ECG)
An EKG is a simple, painless test that records the heart’s electrical activity. It’s the most useful test for diagnosing AF. An EKG shows how fast your heart is beating and its rhythm whether it is steady or irregular. - Standard 12 leads EKG as routinely done in the clinic or hospital.

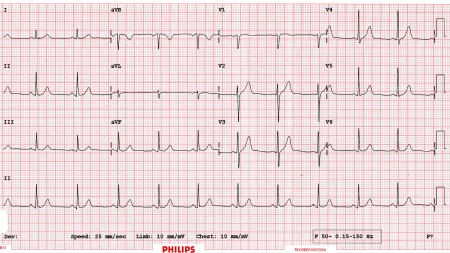
12 Leads ECG of Normal rhythm
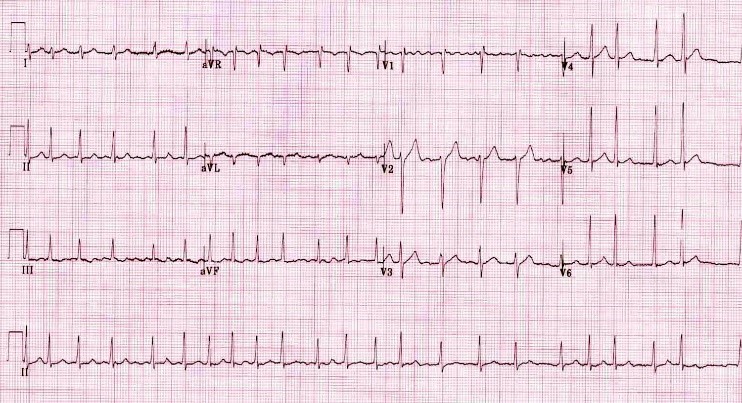
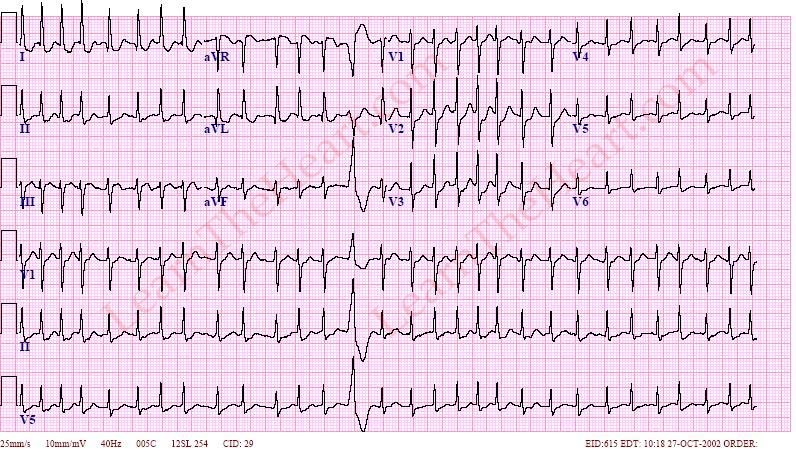
12 Leads ECG of atrial fibrillation


Rhythm strip of normal rhythm

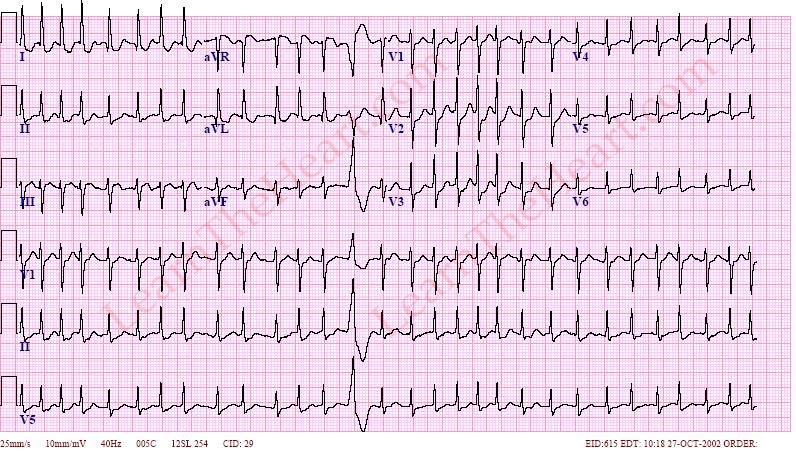
Rhythm strip of atrial fibrillation
Holter and event monitors are portable EKG monitor and can monitor heart electrical activity for a longer period of time. They help diagnosis of paroxysmal AF since a standard EKG only records the heartbeat for a few seconds and miss the AF episode most of the time. - Echocardiography
Transthoracic echocardiography (echo) uses high frequency sound waves to create a moving picture of your heart. The echo is performed by sliding the transducer over the chest where the heart position located. The transducer sends high frequency sound waves through your chest wall to your heart. The sound waves bounce off the structures of your heart, and a computer converts them into pictures on a screen.
The test shows the size and shape of your heart and how well your heart muscle and valves are working. It is also painless and noninvasive (no instruments are inserted into the body).
Echo may identify several heart diseases or conditions that may cause AF or it may reveal the change resulting from AF. - Transesophageal echocardiography (TEE)
The sound wave travels to and fro to the heart through esophageal wall rather through the chest wall. The esophagus is the passage leading from your mouth to your stomach. The esophagus is located right next to the heart and echocardiographic imaging is much clearer.
During this test, the transducer is attached to the end of a flexible tube. The tube is guided down your throat and into your esophagus. You’ll likely be given medicine to help you relax during the procedure.
TEE is used to detect blood clots that may be forming in the atria because of AF. - Chest X Ray
A chest X-ray is a painless test that creates pictures of the structures in your chest, such as your heart and lungs. This test can show fluid buildup in the lungs and signs of other AF complications. - Blood Tests
Blood tests check the level of thyroid hormone in your body and the balance of your body’s electrolytes. Electrolytes are minerals that help maintain fluid levels and acid-base balance in the body. They’re essential for normal health and functioning of your body’s cells and organs.
How is atrial fibrillation treated?
Goals of treatment for atrial fibrillation include:
- Uncover and correct condition that cause or precipitate atrial fibrillation.
- Controlling the heart rate (Rate control)
- Regaining a normal heart rhythm (Rhythm control)
- Preventing blood clots and reducing the risk of stroke (Stroke prevention)
Options to achieve these goals are including lifestyle changes, medications, cardiovertion, catheter-based procedures and surgery. The type of treatment that is recommended is based on the patient heart rhythm, symptoms, type and duration of atrial fibrillation, and other cofounded conditions.
Rate control
Medicines that help slow down the heart rate during atrial fibrillation
- Beta-blockers, preferthe “cardioselective” beta-blockers such as metoprolol, atenolol, bisoprolol.
- Non-dihydropyridine calcium channel blockers such as verapamil or diltiazem.
- Lanoxin is usually not the first or primary choice since it is not effective during exertion
Amiodarone may be considered intravenously in acute situation, when other medication is not suitable.
These medications do not control the heart rhythm (except amiodarone), but do prevent the ventricles from beating too rapidly.
Rhythm control
There are several factors that may influence the recommendation of different mode and timing of rhythm control and the patient should discuss with the doctor in more detail.
Cardioversion is a noninvasive conversion of an irregular heartbeat such as atrial fibrillation to a normal heartbeat using chemical means or electrical.
- Pharmacological cardioversion is performed with drugs, such as propafenone,
flecainide, amiodarone, dronedarone, dofetilide, ibutilide. - Electrical cardioversion is performed by application of direct current electrical shock
Ablation
The procedure involves delivering radiofrequency energy/heat (or other source of energy) through a catheter to eliminate the abnormal area of the heart that causing the atrial fibrillation.
Stroke prevention
Atrial fibrillation is one of the most important causes of stroke. During AF, the heart’s upper chambers, the atria, does not pump. This will cause stasis of the blood and may lead to blood clot formation. If the clot breaks off and travels to the brain, it can cause a stroke. Atrial fibrillation should be taking medication to prevent clot formation, call anticoagulant.
Risk of having a stroke is varied from patient to patient. Guideline has been developed to help anticoagulation management. There are CHADS2 and CHA2DS2-Vas score to help select the patient who should be placed on anticoagulation.
The current oral anticoagulation for long term use in patient with atrial fibrillation are:
Warfarin which is an oral anticoagulant use for several decades. It has been effective in reducing stroke in atrial fibrillation patient, but it is a difficult medicine to use and also include blood test (INR) monitoring.
NOAG (New Oral Anticoagulants) which have been available just in the past few years. This group of medicine is as effective or even better than warfarin but more expensive. They do not need blood test monitoring. They are:
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Elequis)
